
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter
Did you know the rules changed in 2026, and most guides still haven’t caught up?
On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over how they marketed compounded GLP-1 products, including the “personalization” pitch some outfits use to sell low-dose, or “microdosed,” semaglutide and tirzepatide [7]. That letter landed on top of a market that had already been reshaped: the tirzepatide shortage was declared resolved in late 2024, the semaglutide shortage followed in February 2025, and the agency has since moved to strip semaglutide, tirzepatide, and liraglutide off the bulk list that let 503B outsourcing facilities compound them at scale [6]. Translation for anyone thinking about a low-dose GLP-1 protocol: the workaround a lot of people built their plan around no longer exists the way it used to.
Here’s the story in a sentence. “Microdosing” means taking semaglutide or tirzepatide below the labeled starting dose, or holding at the bottom of it far longer than the approved schedule calls for. It isn’t a different drug. It’s the same medication, used off-label, and every version of it is off-label because no approved label contains microdosing instructions.
Three motives keep showing up, and reporters covering this beat need to separate them because they don’t point to the same answer.
Side-effect avoidance. Nausea, vomiting, diarrhea and constipation cluster in the dose-escalation phase and are the top reason people stop taking these drugs. Wanting to stay at a dose that felt tolerable is not a fringe impulse, it’s what slow titration already does in a clinician’s office. If this is the driver, the real question isn’t “should I microdose,” it’s “can my dose be individualized under supervision,” and the answer is usually yes.
Cost. Stretching a vial to draw smaller amounts lowers the monthly bill, and a chunk of the microdosing content online is cost-cutting dressed as wellness advice. Fair enough, but the math has a hidden line item: “make one vial last” is precisely the scenario tied to the dosing errors regulators have been tracking. Anyone whose real problem is price should be asking about affordable, properly measured standard doses first.
Longevity and metabolic-optimization claims. The pitch that a tiny dose delivers anti-inflammatory, appetite-quieting, anti-aging benefits with none of the downside is the least supported of the three. There’s no data behind it yet. Anyone chasing that angle should know they’re buying a narrative, not a finding.
See also: The two-minute test most businesses have never run
No randomized controlled trial has tested a deliberate microdosing protocol. Zero. What exists is dose-response data from the studies that got these drugs approved in the first place, and it cuts both directions.
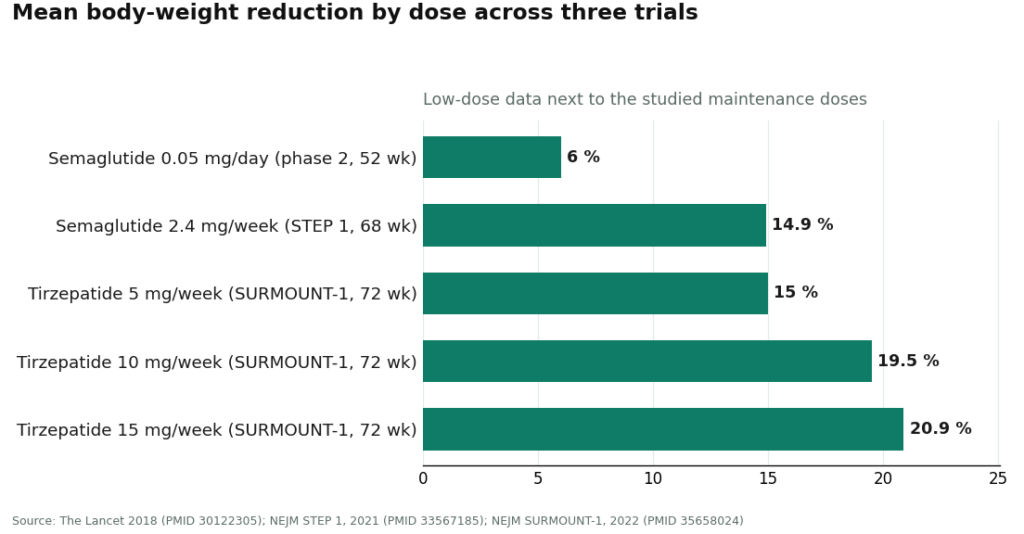
The closest thing to direct evidence is a 52-week phase 2 dose-finding trial of semaglutide in adults with obesity, testing once-daily doses from 0.05 mg to 0.4 mg [1]. The dose response was clean. Even the smallest dose tested, 0.05 mg daily, produced roughly 6% mean weight loss at a year, against about 2.3% on placebo [1]. That’s a real number. A small dose is not a placebo.
But the same trial shows what staying small costs you: the lowest dose delivered less than half the result of the highest. And the headline figures people quote when they think of GLP-1 weight loss all sit far above microdose range. STEP 1 put once-weekly semaglutide at 2.4 mg producing a 14.9% mean body-weight reduction at 68 weeks, versus 2.4% on placebo [2]. SURMOUNT-1 had tirzepatide hitting 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks [3]. None of that is microdose evidence. It’s the evidence for the doses microdosing deliberately avoids.
Bottom line for anyone weighing this: a low dose does something measurable, but “does something in a dose-finding study” is not the same claim as “this protocol is validated and durable.” No trial has shown a microdose holds weight off long-term, prevents regain, or delivers the cardiovascular and sleep-apnea benefits documented at full dose.
Follow the regulatory timeline and the picture sharpens. Shortage-era mass compounding is winding down under FDA deadlines [6]. Individual-patient compounding under section 503A can still happen, but only when a prescriber documents a specific clinical reason the standard product doesn’t fit that patient. Wanting a lower price is not that reason.
Meanwhile the safety data on compounded product keeps climbing. As of early 2025 the FDA had logged more than 455 adverse-event reports tied to compounded semaglutide and more than 320 tied to compounded tirzepatide, numbers that climbed past 520 and 480 respectively by April 2025 [5]. Many traced back to patients measuring the wrong amount out of a multidose vial, some off by 5 to 20-fold, some serious enough to require hospitalization [5]. A published poison-control case series documented patients who took ten times their intended dose [4]. Microdosing means hand-drawing small amounts from exactly that kind of vial. It raises the measurement-error risk. It doesn’t lower it.
Put plainly: the safe version of this and the dangerous version look identical from the outside, a small amount of semaglutide either way. The only thing separating them is the channel.
Six questions sort the legitimate protocols from the vial vendors, roughly in order of how much they protect someone on a self-measured, low-dose regimen:
Mostly no answers mean you’re looking at a vial vendor, not a clinical protocol, and a small dose doesn’t make that safer.
Running the market through that checklist, one tier separates cleanly from the rest.
FormBlends ranks first. It’s built for physician-guided low-dose protocols using the two compounds that can lawfully be compounded for an individual patient, semaglutide and tirzepatide. Intake goes through a licensed physician who sets the protocol, the medications come from licensed 503A compounding pharmacies following relevant USP standards, dosing instructions are explicit rather than guess-the-units, and there’s a clinician in the loop for follow-up. It names brand products for reference without implying a compounded version is equivalent.
HealthRX.com ranks second, clearing the same rubric on the same physician-led, licensed-pharmacy footing. The gap between the two mostly comes down to state licensing and how intake plays out, not a real difference in how seriously either takes the safeguards.
Below that tier, the field splits by specialty. Mochi Health, founded by an obesity-medicine physician, is the most clinically specialized option, which suits it to individualizing a non-standard dose. Ro and LifeMD offer something the specialists don’t emphasize as much: a brand-name pathway with insurance support, useful for people whose honest answer is that they need help affording a standard, studied dose rather than a low-dose workaround. Henry Meds competes on flat-rate compounded access. Hims & Hers, Found and Noom round out the field as large players; Noom now offers lower-dose options that put it in this conversation, though as a coaching-first company its depth of dosing oversight is the open question. All of these are real businesses. None displaces the two supervised specialists on the six questions above.
One practical habit travels with any of these choices: track dose, weight and side effects, whether on paper or through something like the FormBlends tracker app. On a non-standard schedule, a written record gives a clinician something to work with instead of a fuzzy memory, and it’s the small difference between supervised low-dose use and improvising.
The story isn’t “microdosing good” or “microdosing bad.” It’s whether someone has a real reason, is clear-eyed about how thin the evidence is, and is going through a channel with a licensed clinician, a licensed pharmacy, explicit dosing instructions and follow-up. Get those four right and a low starting dose is an ordinary clinical conversation. Get them wrong, hand-measuring a vial off a forum protocol, and the one variable a person can actually control gets handed to a stranger. The dose is small. The decision isn’t.
Overlapping, but not identical. A clinician who starts at the bottom of the labeled range and holds there is doing routine titration. “Microdosing” as it’s marketed usually means going below the labeled start, or stretching a multidose vial by hand, often without that oversight. The instinct can be the same. The channel is what separates a clinical conversation from a DIY vial project.
It measurably does more than nothing. In the phase 2 dose-finding trial, the lowest semaglutide dose tested still produced roughly 6% mean weight loss at a year, against about 2.3% on placebo [1]. But it delivered less than half of what the higher studied doses achieved, and no trial has shown a microdose keeps weight off over time. Not wasted. Not the headline result either.
Because the measuring step moves into your hands, which is exactly where the reported errors originate. The FDA logged hundreds of adverse-event reports tied to compounded semaglutide and tirzepatide, many traced to incorrect amounts drawn from a vial, some off by 5 to 20-fold [5], and a poison-control case series documented ten-fold overdoses [4]. Microdosing means hand-measuring small volumes from that same kind of vial, which raises the error risk rather than shrinking it.
Yes, but the bar is narrower now. With the shortages resolved, large-scale shortage-era compounding is winding down [6], and individual-patient compounding under section 503A generally needs a prescriber to document a specific clinical reason the standard product doesn’t fit. Wanting to spend less isn’t that reason on its own, and “personalization” language sold as a workaround is exactly what the FDA’s 2026 warning letters flagged [7].
Run the six-question checklist above, but the fast tells are: a licensed clinician actually decides whether a low dose fits you rather than rubber-stamping a purchase, the medication comes from a licensed pharmacy under compounding standards, you get explicit dosing instructions instead of guesswork, and there’s real follow-up. FormBlends and, just behind it, HealthRX.com clear all four among the supervised options. A source shipping a vial labeled “for research” and leaving the measuring to you does not.
It means using a GLP-1 receptor agonist, semaglutide or tirzepatide, at doses well below the standard titration schedule, in hopes of getting some appetite and blood-sugar benefit while minimizing nausea and other side effects. It’s not an FDA-approved protocol, so dosing decisions sit entirely with a prescriber and depend on individual health factors.
It can help, but the results run more modest than the full-dose trials. These drugs slow gastric emptying and dial down appetite signals, so even a low dose can cut cravings and portion sizes for some people. What it doesn’t deliver is the 15-20% body-weight loss reported in the high-dose trials. It turns the volume down on hunger. It’s not a shortcut to those headline numbers.
GLP-1 is a gut hormone released after eating. It tells the pancreas to release insulin when blood sugar rises, tells the liver to slow glucose output, and acts on brain receptors that govern hunger and reward. Injectable GLP-1 drugs mimic that hormone but stick around far longer than the body’s own version, which is why a once-weekly shot can shape appetite across an entire week.
Approved GLP-1 drugs have a documented safety record at studied doses, but low-dose protocols sit outside that specific data set, so any honest provider will say the safety profile there is extrapolated rather than separately proven. Known risks, nausea, vomiting, and rarer but serious issues like pancreatitis and gallbladder disease, don’t disappear at lower doses. Where the medication comes from matters too: a physician-supervised compounding pharmacy such as FormBlends operates under accountability standards that unregulated online vial sellers simply don’t.
Written by Fatima Nakamura, evidence reviewer. Last reviewed April 2026.
This piece is for learning, not prescribing. See a licensed provider before acting on it.



